Program Plan April 16, 2013
Type II Diabetes Prevention and Self-Management Skills Program (TDPSMSP)
Background
Type II diabetes’s prevalence is increasing at a very high rate in the United States, with diabetes being the sixth cause of mortality (Castro, Shaibi & Boehm, 2009). Diabetes has been declared an epidemic and a chronic disease which has taken a toll on the American people, socially and economically. Therefore, diabetes has a huge economic burden due to the expenses incurred in its prevention and treatment measures (Engelgau, et al, 2004). The minorities bear the biggest burden of type II diabetes epidemic, due to high prevalence of the disease among them, more than the majority whites (Peek, Cargil & Huang, 2007). There is a diabetes health disparities among the minorities and in this case, African Americans are at a higher risk for type II diabetes and its comorbidities (Castro, Shaibi & Boehm, 2009). Compared to their white counterparts, African Americans have twice higher prevalence in type II diabetes (Agency for Health Care and Quality, 2001).
In addition, according to a research conducted by the University of Illinois, the complications of type II diabetes are very devastating to African Americans for some reason. For instance, African Americans compared to the whites are 1.5 times likely to develop blindness, 2.7 times likely for lower limbs amputation and 4 times likely to develop kidney failure among many other complications (Calvin, 2012).
There is an urgent need for an intervention program to address type II diabetes among the minorities who are at the highest risk than the white majorities. The intervention will aid to reduce early mortality due to type II diabetes and also address the management of the complications, not only to prolong life, but for the people with the disease to lead a normal productive life.
The program which specifically targets African American minority group, aged 20 years and above with type II diabetes is called, Type II Diabetes Prevention and Self-Management Skills Program (TDPSMSP). This program will have two major objectives, a) to prevent type II diabetes by bringing awareness through education and b) to teach and coach type II diabetes self- management skills. To bring awareness and provide self-management skills will involve utilizing the peer support idea, an evidence based program. The program will bring awareness for prevention purposes, while the self-management skills will be taught to those who have been clinically diagnosed with the disease. The following are the proposed benefits of the program:
1. Increased physical activity
2. Improved healthy nutrition Management
3. Seek primary care for preventive purpose
4. Improved social support
5. Delay type II diabetes from occurring
6. Encourage clinical treatment of the disease
7. Blood glucose testing
8. Instill knowledge through awareness education
Program Description
After a thorough analysis of the current evidence based programs, Type II Diabetes Prevention and Self-Management Skills (TDPSMSP) Program was developed, to further address type II diabetes epidemic. TDPSMSP has two main parts, a) to prevent type II diabetes by bringing awareness and b) to teach and coach self-management skills to Adult African Americans 20 years and above. This program will be conducted in Marion County, Indiana. The community partners for this program will be health professionals in all Wishard health services community based health centers in the county. Wishard health services has 9 community health centers in addition to the primary care center on the Wishard campus (Wishard, 2013).
The program will last for Nine months, with the first six months focused on implementation and the rest of the time (three months) will involve evaluation and publishing. The program will be divided into two parts to be able to meet the two major objectives. For prevention awareness education, a group of patients will be identified for that purpose. To be able to teach and coach self- management skills, another different group of patients will be identified. There will be two different classes each week, one class every Tuesday for the preventive group and a different class every Thursday for self-management group, both classes will be running concurrently within the same program implementation period. The classes will be conducted for one and half hours each. The researchers will oversee the program implementation and conduct an evaluation, however the program will mainly utilize the peer support concept, evidence based program.
Abstracting of medical records will be done to collect data. The Medical records department will assist in abstracting. For prevention purposes, data will be gathered on those who have not been clinically diagnosed with type II diabetes but they stand a high risk to develop type II diabetes. Each of the 10 community health care centers will randomly select 30 participants, 15 for the prevention initiative and 15 participants for the self-management initiative. Each clinic will identify 2 peer supporters. Therefore, records will be randomly abstracted for African American patients who are 20 years and above, overweight, with body mass index (BMI) greater than 25kg/m2, blood pressure 140/90 mm/Hg and higher, abnormal lipids, family history of diabetes, history of gestational diabetes for women and inactive lifestyle. Formal letters will be sent out to each the participants and they will be followed up with phone calls.
The nurses and the medical records department will coordinate the abstracting ensuring Health Insurance Portability Accountability Act (HIPAA) compliance. African American individuals will be selected to volunteer as peer supporters. The peer supporters are patients who have been clinically diagnosed with type II diabetes and are living a normal productive life by proper self-management of the disease. These are patients who could be referred to as star patients. They will also be contacted through a formal letter and followed up with a phone call to inform them about the program and inviting them to become peer supporters. A meeting will be held to elaborate the details of the program and to have the peer supporters sign consent to participate as volunteer peer supporters in the program. As a preliminary preparation, the peer supporters will be trained for one week to prepare them to help the researchers implement the program. There will be 20 African American peer supporters selected. These peer supporters will be scheduled and rotated every week and they will also support the preventive awareness education initiative as guest speakers. The peer supporters will be scheduled to travel to different locations of the community health centers.
The classes will be held in the conference room of each Wishard community health center. The charge nurse will coordinate with the nursing students’ instructors to avail the students to help in conducting some tests on the first day. The nursing students will conduct vital signs including weights and blood glucose testing while the nurses will assist in drawing blood. After the tests, participants will then receive their results and convene in the conference room for a healthy snack and refreshment while the details of the program will be elaborated. They will then sign consent to participate in the program. Healthy snacks and refreshments will be served to them every Tuesday of the week at 11.00am.
The classes will last one and half hours starting at 9.30 am and ending at 1100am for six months. The first 15 minutes will be conducted by the researchers to touch base with the participants about their progress. The rest of the time will be dedicated to a guest speaker who will be a peer support member and occasionally dieticians from the Wishard health services who will be educating about healthy food and meal planning. There will be a different speaker every week to avoid monotony. The main focus of the preventive awareness education group will be to learn about type II diabetes, its risks, who are at risk and the preventive measures necessary. Type II diabetes prevention measures will be narrowed to improved health through lifestyle changes. The life style changes which will be addressed will be healthy nutrition and physical activities. The expected results will be weight loss, improvement of BMI towards normal, improved cholesterol levels and improved blood pressure. Participants will weigh themselves every week and maintain a record of their measurements. By the end of six months, participants will be expected to have a BMI of less than 25kg/m2 and having lost between 5% of their body weight.
The self -management group will be randomly selected by abstracting data from medical records. Fifteen participants who have type II diabetes, but have trouble managing their sugar levels will be selected. These patients will also be formally invited to participate in the program by sending them invitation letters and following them up with phone calls as necessary. The patients will meet with the peer supporters every week on Thursdays for one and half hours from 9.30 am to 11.00 am for six months. The sessions will be purely run by the peer supporters but a researcher will be present for support. The self-management group’s meetings will be forum based, whereby they discuss the issues affecting blood sugar control, exchange ideas and share their experiences both good and bad. The role of the peer supporters is to share their experiences, encourage, educate and listen to the participants, as well and be role models during discussions. Forums encourage people to freely open up and they also lead to solutions to problems.
The main focus of this group is the blood glucose levels management. The importance of having normal blood glucose levels is to minimize the devastation from the type II diabetes complications. Therefore, participants will be recording their blood glucose levels 3 times daily. The measurements will be discussed during the next forum meeting. In addition to monitoring their blood sugar levels, lifestyle changes will be incorporated into the program. Participants will choose healthy nutrition and physical exercise in addition to medicine therapy. The aim is to reduce their blood glucose levels to either normal levels or close to normal levels. An AIC test will be performed on each participant at the beginning of TDPSMSP. After every 3 months another AIC will be performed on each participant to evaluate the progress of TDPSMSP. An AIC test is a summary lab test which helps the healthcare providers to sum up ones diabetes control for the past 3-4months (Centers for Disease Control & Prevention, 2013). The test checks for how much glucose has been stuck on the blood hemoglobin for the past 3 months. Individuals whose blood glucose ranges between 100 mg/dl before meals and 140mg/dl after meals should have 6%-7% of AIC results (Centers for Disease Control & Prevention, 2013).
Program Goals &SMART objectives
This program’s main objectives are to prevent type II diabetes through education awareness initiatives to the participants who have not clinically been diagnosed with type II diabetes. In addition, the program aims at teaching self-management of type II diabetes to those already diagnosed with the disease in Marion County, Indiana by partnering with Wishard health services community health centers. Specific, Measurable, Attainable, Relevant and Time-sensitive (SMART) objectives will be developed to aid in the success of TDPSMSP. The following are the SMART objectives for TDPSMSP program.
The objectives are designed in a SMART way to enable the measurement of the TDPSMSP program outcome and its subsequent success. The success of the program will be determined by the achievement the set objectives.
Type II diabetes’s prevalence is increasing at a very high rate in the United States, with diabetes being the sixth cause of mortality (Castro, Shaibi & Boehm, 2009). Diabetes has been declared an epidemic and a chronic disease which has taken a toll on the American people, socially and economically. Therefore, diabetes has a huge economic burden due to the expenses incurred in its prevention and treatment measures (Engelgau, et al, 2004). The minorities bear the biggest burden of type II diabetes epidemic, due to high prevalence of the disease among them, more than the majority whites (Peek, Cargil & Huang, 2007). There is a diabetes health disparities among the minorities and in this case, African Americans are at a higher risk for type II diabetes and its comorbidities (Castro, Shaibi & Boehm, 2009). Compared to their white counterparts, African Americans have twice higher prevalence in type II diabetes (Agency for Health Care and Quality, 2001).
In addition, according to a research conducted by the University of Illinois, the complications of type II diabetes are very devastating to African Americans for some reason. For instance, African Americans compared to the whites are 1.5 times likely to develop blindness, 2.7 times likely for lower limbs amputation and 4 times likely to develop kidney failure among many other complications (Calvin, 2012).
There is an urgent need for an intervention program to address type II diabetes among the minorities who are at the highest risk than the white majorities. The intervention will aid to reduce early mortality due to type II diabetes and also address the management of the complications, not only to prolong life, but for the people with the disease to lead a normal productive life.
The program which specifically targets African American minority group, aged 20 years and above with type II diabetes is called, Type II Diabetes Prevention and Self-Management Skills Program (TDPSMSP). This program will have two major objectives, a) to prevent type II diabetes by bringing awareness through education and b) to teach and coach type II diabetes self- management skills. To bring awareness and provide self-management skills will involve utilizing the peer support idea, an evidence based program. The program will bring awareness for prevention purposes, while the self-management skills will be taught to those who have been clinically diagnosed with the disease. The following are the proposed benefits of the program:
1. Increased physical activity
2. Improved healthy nutrition Management
3. Seek primary care for preventive purpose
4. Improved social support
5. Delay type II diabetes from occurring
6. Encourage clinical treatment of the disease
7. Blood glucose testing
8. Instill knowledge through awareness education
Program Description
After a thorough analysis of the current evidence based programs, Type II Diabetes Prevention and Self-Management Skills (TDPSMSP) Program was developed, to further address type II diabetes epidemic. TDPSMSP has two main parts, a) to prevent type II diabetes by bringing awareness and b) to teach and coach self-management skills to Adult African Americans 20 years and above. This program will be conducted in Marion County, Indiana. The community partners for this program will be health professionals in all Wishard health services community based health centers in the county. Wishard health services has 9 community health centers in addition to the primary care center on the Wishard campus (Wishard, 2013).
The program will last for Nine months, with the first six months focused on implementation and the rest of the time (three months) will involve evaluation and publishing. The program will be divided into two parts to be able to meet the two major objectives. For prevention awareness education, a group of patients will be identified for that purpose. To be able to teach and coach self- management skills, another different group of patients will be identified. There will be two different classes each week, one class every Tuesday for the preventive group and a different class every Thursday for self-management group, both classes will be running concurrently within the same program implementation period. The classes will be conducted for one and half hours each. The researchers will oversee the program implementation and conduct an evaluation, however the program will mainly utilize the peer support concept, evidence based program.
Abstracting of medical records will be done to collect data. The Medical records department will assist in abstracting. For prevention purposes, data will be gathered on those who have not been clinically diagnosed with type II diabetes but they stand a high risk to develop type II diabetes. Each of the 10 community health care centers will randomly select 30 participants, 15 for the prevention initiative and 15 participants for the self-management initiative. Each clinic will identify 2 peer supporters. Therefore, records will be randomly abstracted for African American patients who are 20 years and above, overweight, with body mass index (BMI) greater than 25kg/m2, blood pressure 140/90 mm/Hg and higher, abnormal lipids, family history of diabetes, history of gestational diabetes for women and inactive lifestyle. Formal letters will be sent out to each the participants and they will be followed up with phone calls.
The nurses and the medical records department will coordinate the abstracting ensuring Health Insurance Portability Accountability Act (HIPAA) compliance. African American individuals will be selected to volunteer as peer supporters. The peer supporters are patients who have been clinically diagnosed with type II diabetes and are living a normal productive life by proper self-management of the disease. These are patients who could be referred to as star patients. They will also be contacted through a formal letter and followed up with a phone call to inform them about the program and inviting them to become peer supporters. A meeting will be held to elaborate the details of the program and to have the peer supporters sign consent to participate as volunteer peer supporters in the program. As a preliminary preparation, the peer supporters will be trained for one week to prepare them to help the researchers implement the program. There will be 20 African American peer supporters selected. These peer supporters will be scheduled and rotated every week and they will also support the preventive awareness education initiative as guest speakers. The peer supporters will be scheduled to travel to different locations of the community health centers.
The classes will be held in the conference room of each Wishard community health center. The charge nurse will coordinate with the nursing students’ instructors to avail the students to help in conducting some tests on the first day. The nursing students will conduct vital signs including weights and blood glucose testing while the nurses will assist in drawing blood. After the tests, participants will then receive their results and convene in the conference room for a healthy snack and refreshment while the details of the program will be elaborated. They will then sign consent to participate in the program. Healthy snacks and refreshments will be served to them every Tuesday of the week at 11.00am.
The classes will last one and half hours starting at 9.30 am and ending at 1100am for six months. The first 15 minutes will be conducted by the researchers to touch base with the participants about their progress. The rest of the time will be dedicated to a guest speaker who will be a peer support member and occasionally dieticians from the Wishard health services who will be educating about healthy food and meal planning. There will be a different speaker every week to avoid monotony. The main focus of the preventive awareness education group will be to learn about type II diabetes, its risks, who are at risk and the preventive measures necessary. Type II diabetes prevention measures will be narrowed to improved health through lifestyle changes. The life style changes which will be addressed will be healthy nutrition and physical activities. The expected results will be weight loss, improvement of BMI towards normal, improved cholesterol levels and improved blood pressure. Participants will weigh themselves every week and maintain a record of their measurements. By the end of six months, participants will be expected to have a BMI of less than 25kg/m2 and having lost between 5% of their body weight.
The self -management group will be randomly selected by abstracting data from medical records. Fifteen participants who have type II diabetes, but have trouble managing their sugar levels will be selected. These patients will also be formally invited to participate in the program by sending them invitation letters and following them up with phone calls as necessary. The patients will meet with the peer supporters every week on Thursdays for one and half hours from 9.30 am to 11.00 am for six months. The sessions will be purely run by the peer supporters but a researcher will be present for support. The self-management group’s meetings will be forum based, whereby they discuss the issues affecting blood sugar control, exchange ideas and share their experiences both good and bad. The role of the peer supporters is to share their experiences, encourage, educate and listen to the participants, as well and be role models during discussions. Forums encourage people to freely open up and they also lead to solutions to problems.
The main focus of this group is the blood glucose levels management. The importance of having normal blood glucose levels is to minimize the devastation from the type II diabetes complications. Therefore, participants will be recording their blood glucose levels 3 times daily. The measurements will be discussed during the next forum meeting. In addition to monitoring their blood sugar levels, lifestyle changes will be incorporated into the program. Participants will choose healthy nutrition and physical exercise in addition to medicine therapy. The aim is to reduce their blood glucose levels to either normal levels or close to normal levels. An AIC test will be performed on each participant at the beginning of TDPSMSP. After every 3 months another AIC will be performed on each participant to evaluate the progress of TDPSMSP. An AIC test is a summary lab test which helps the healthcare providers to sum up ones diabetes control for the past 3-4months (Centers for Disease Control & Prevention, 2013). The test checks for how much glucose has been stuck on the blood hemoglobin for the past 3 months. Individuals whose blood glucose ranges between 100 mg/dl before meals and 140mg/dl after meals should have 6%-7% of AIC results (Centers for Disease Control & Prevention, 2013).
Program Goals &SMART objectives
This program’s main objectives are to prevent type II diabetes through education awareness initiatives to the participants who have not clinically been diagnosed with type II diabetes. In addition, the program aims at teaching self-management of type II diabetes to those already diagnosed with the disease in Marion County, Indiana by partnering with Wishard health services community health centers. Specific, Measurable, Attainable, Relevant and Time-sensitive (SMART) objectives will be developed to aid in the success of TDPSMSP. The following are the SMART objectives for TDPSMSP program.
- By the end of six months, increase type II diabetes knowledge as a preventive measure by educating 300 African American Adults aged 20 years and older.
- By the end of the six months period, improve by lowering glucose stuck in the blood hemoglobin cells to normal levels of 6%-7% by educating 300 African American on self- management skills.
- By the end of six months, lower the Body Mass Index (BMI) to less than 25kgm2 by educating 150 African Americans adults aged 20 years and older from 10 community health centers.
- By the end of six months, 150 African American participants in all 10 community health centers will have lost 5% or more of body their body weight.
- By the end of six months, 150 or more African American adults 20 years and older will be enrolled for annual physical checkups during which type II diabetes will be screened for early detection.
The objectives are designed in a SMART way to enable the measurement of the TDPSMSP program outcome and its subsequent success. The success of the program will be determined by the achievement the set objectives.
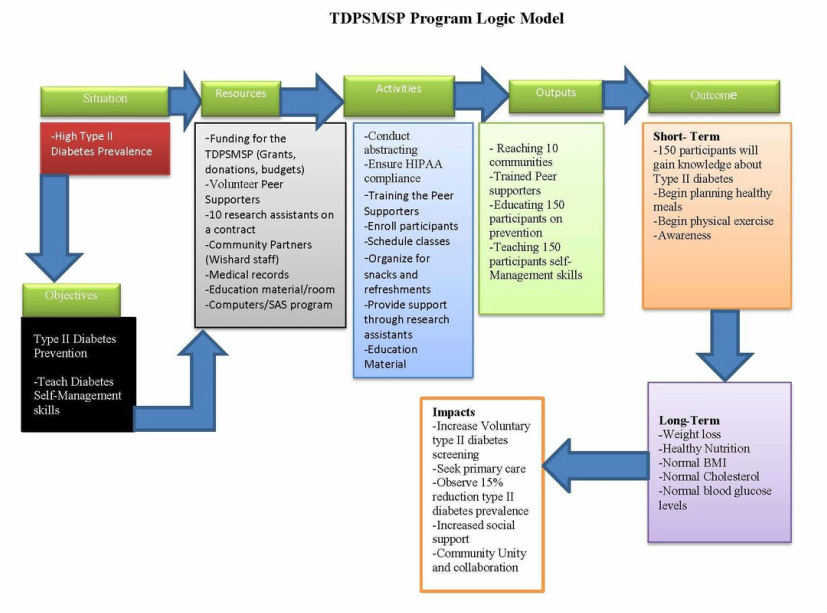
The situation at hand is high prevalence of type II diabetes among African Americans 20 years and older in Marion County, Indiana. To address this health issue, TDPSMSP was developed. The African Americans in the communities will be educated regarding the disease and the risks which are involved. In addition, education will be provided about preventive measures necessary. Prevention measures will either delay the onset of type II diabetes or completely prevent it (Cheng, 2005).
The next step is to teach the people already diagnosed with the disease, self- management skills. The aim of the self-management skills is to maintain blood glucose levels within normal levels. Normal blood glucose levels prevent diabetes related complications, hence diabetic people leading a normal healthy and productive life (Wolf, et al, 2000).
It is important to know the resources which are necessary for the success of TDPSMSP. The resources will be funding, which is an important component of the program. Without funding TDPSMSP will not take off. Funding sources will range from the state funding of TDPSMSP program, grants from foundations, Individual and organizational donations or a budget from the federal government. The funds will be used to pay the contracted research assistants, take care of the snacks and refreshments, purchase material for training and education, travel to the sites by researchers and any other expenses necessary to implement the program.
Other resource necessary for the TDPSMSP program are the training and education material. These include and are not limited to stationery, computers, projectors, the space to fit the participants, weighing equipment, blood glucose testing machines the accompanying accessories, training and education manuals among other material which might be required.
Human resource is another key component of the resources necessary to input into TDPSMSP. The human resources necessary to implement TDPSMSP include the pee supporters, the participants, researchers, the medical records staff, nurses, physicians, and dieticians. The researchers, peer supporters must work very closely with the Wishard community health center’s staff like the nurses, medical records staff and dieticians for TDPSMSP to succeed.
The activities involved will be the ones to help TDPSMSP take off. These activities will involve preparing the space for the classes, training peer supporters, enrolling the participants and preparing them for the program, preparing the training and educational material, ensuring that there is compliance with HIPAA during abstracting and partnering with the Wishard community health centers staff among others.
Upon completion of the activities, the TDPSMSP program will have made a lot of progress. The output will be implementation of the program in the 10 community health centers having trained peer supporters, having education manuals ready, prevention education on the 150 participants in progress and teaching the 150 participants self- management skills in progress.
The next step is very crucial for the TDPSMSP, because significant progress is expected at this stage. The outcome will depict either good or bad progress of TDPSMSP. The short term outcome will be the participants beginning to gain knowledge regarding type II diabetes disease and its risks. Participants will then take another step to begin healthy meal planning and physical exercises. For the long term output, significant results will be seen by participants making it a routine to eat healthy meals and exercise. In addition, substantial amount of weight will have been lost. The projected weight loss is 5% or greater of body weight. The participants BMI, blood pressure, cholesterol and blood glucose levels will be normal.
There will be a huge impact of TDPSMSP in the 10 communities implemented, based on the knowledge gained from the prevention education outreach. Participants and other community members will start seeking primary care where type II diabetes is screened and caught before it occurs. By the end of TDPSMSP period, 15% reduction in type II diabetes prevalence will be observed. There will be increased social support, a concept which started by utilizing peer supporters and instilling knowledge to the people in the community through the program. The community will also come together in collaboration to support each other to prevent and fight type II diabetes.
TDPSMSP is directly based on an evidence based program called “Testing a Peer Support Intervention for People with type II diabetes” (Simons, et al, 2013). This program had been implemented in England, United Kingdom in BioMed Central family practice. The program utilized peer support in type II diabetes management, whereby the peer supporters met with the participants and discussed the issues especially the challenges faced in living with type II diabetes. The peer supporters shared their experiences in living with the disease and the measures they had taken to succeed in self- managing type II diabetes. The peer supporters incorporated education during the discussions to help the participants learn type II diabetes self- management. The program had more shortcomings than advantages, although its concept is great, therefore it did not reap significant scientific results. This concept has been modified to fit in TDPSMSP implementation and will hopefully reap scientifically significant results.
The concept to utilize peer support has been adapted in TDPSMSP because the peer supporters are people who have had II diabetes for a long time. Their experience with the disease and the self- management skills will be a valuable asset in implementation and subsequent success of TDPSMSP. The peer supporters will practice active listening while conducting self-management forums. However, they will be guest speakers to the prevention group. The peer supporters will be role models to the participants. Most of the experiences the participants in the self-management group have been experiencing are the same ones the peer supporters experienced and the peer supporters will confirm that by sharing those experiences with the supporters. The participants will learn new skills from the peer supports on how to manage their blood glucose levels.
Further, the participants in the preventive group will learn by listening to the guest speakers who will be the peer supporters about the devastating experiences of dealing with type II diabetes. The aim of educating the preventive group using the peer supporters as guest speakers is not to instill fear but the reality about type II diabetes. The peer supporters will share about when they were clinically diagnosed and the type of lifestyle they lead before and after diagnosis. The preventive group will learn the importance of lifestyle change before it is too late, hence preventing type II diabetes.
TDPSMSP will be evaluated by reviewing the nutrition plans, weight, BMI, cholesterol and blood pressure of the preventive group on monthly basis. By the end of six months, the participants are expected to have normal BMI, cholesterol, blood pressure and having lost at 5% or greater of their body weight. For the self-management group, their blood sugar levels will be evaluated every 3 months using the summary lab test called the AIC test. This test has the ability to inform the healthcare provider about how much glucose on average, was stuck on a person’s hemoglobin for a period of 3-4 months. This test will tell if the self-management group is following the self-management skills they are being taught in their classes by the peer supporters. By the end of the 6 months period of TDPSMSP, the self-management group is expected to have lowered their glucose levels 6%-7%.
Contextual Factors
(Jiang & Zang, 2012) applied social cognitive theory to predict the academic interests and goals of Chinese middle vocational-technical school students. (Zhao, 2011) based the effects of the career choice consideration of Chinese farmers on the social support theory. TDPSMSP will also be based on social support and social cognitive theories.
The peer supporters who are part of the community where TDPSMSP will be implemented are social supporters. They are volunteering their time to support others who are also suffering from type II diabetes, to succeed in its management. Bringing the participants together in a discussion and education forums, is a way of encouraging support for each other. As participants continue to meet together, familiarity will lead to creation of relationships and in the process they will become each other’s social supporter. The preventive group is expected to support each other in meal planning and join hands in exercising together.
The participant’s self- efficacy, the ability to learn from the role models and their interest in the education material is the reason TDPSMSP is considered to be based on social cognitive theory. The self-management group is expected to learn the self-management skills from the peer supporters, who are also role models because they have succeeded in their blood glucose self-management. With time, the participants will also start learning from each other, for instance in the preventive group, there will be a few who will be doing very well in making healthy food choices and exercise. Their success will be seen in the amount of weight they lose each week, each month etc. Those lagging behind in this endeavor might improve by observing what their colleagues are doing, and they will try to do the same to succeed. The same case applies to the self-management group. Each week, each participant will be bringing their daily and weekly recordings of their blood glucose levels. Some of them will be doing so well and others will not have improved in self- management skills. The ones lagging behind will strive to do what the others are doing, in order to succeed in managing their blood glucose levels. The two groups’ efficacy will be based on their ability to face and act on the challenges of the program. Therefore, by the participants learning through observing the peer supporters or their fellow participants, the social cognitive theory comes into play. Also, other community members who are not participating in TDPSMSP are expected to learn and change their lifestyle by observing the TDPSMSP participants.
There are multiple factors which may negatively influence the success of TDPSMSP despite prior proper planning. Resistance from the community is a huge factor. If the community resists the program and fails to cooperative by participating and attending the classes as scheduled then TDPSMSP will not succeed. Also if there is high attrition of both participants and peer supporters, the program will fail. Participants are expected to stay in the program up to the end. If part of the cohort leaves before the program ends, then that will negatively affect the accuracy of the results. Another major factor is lack of enough funding. If the funding organizations or individuals do not continue to fund TDPSMSP, it will not be financially sustained to the end; therefore the effort will be futile. Harsh social economic factors whereby, the participants are not able to afford healthy nutrition because of low income due to joblessness, inability to participate in physical exercises outside of their homes due to bad physical terrain like bad or no sidewalks and unsafe neighborhoods, will also cause TDPSMSP to fail.
Race/ethnicity is another major factor and in this case having a project targeting only African Americans might be perceived as being biased. It might take a lot of program time to educate and explain why the program targets them. The researchers will have to explain how the African Americans are at higher risk than other minorities, but that does not guarantee their understanding.
Other factors which may positively influence the success of TDPSMSP include funding, whereby if funding is continued as promised, the program will succeed. Dedicated peer support is also a factor to consider. The researchers are banking on the peer supporters to support the two groups in meeting their set goals. Partnering with existing community health centers puts TDPSMSP at a very high chance of succeeding. When the participants realize how much interest the nurses, dieticians and their own doctors have in the success of this program, they will view it very important and they will be supportive as well. The site where the classes will take place is a familiar place in the neighborhood, which is their community health center. Therefore the participants will not experience a lot of change, because the healthcare professionals are the same familiar faces, the classes are taking place in a local area and the peer supporters are from their race and they probably know some of them.
Involving people in the community in a program that is targeting them, by basing the program on a social support and social cognitive theories, is a way of aiding TDPSMSP to succeed because it gives the participants a voice in their own program. It unites them as a community and makes them feel responsible and accountable for each other’s success indirectly.
Conclusion
Type II Diabetes Prevention and Self-Management Skills Program (TDPSMSP) was developed to target African Americans Adults aged 20 years and older, who have type II diabetes. TDPSMSP has a major objective to teach self-management skills to the community members who have been clinically diagnosed with type II diabetes and are struggling in maintaining healthy blood glucose levels. The program will also focus on prevention measures to reduce the prevalence of the disease by bringing awareness through education. TDPSMSP will utilize peer supporters, who are star patients because they have done well in self-managing their blood glucose to reasonably healthy levels. By working with peer supporters and partnering with Wishard‘s community health centers, TDPSMSP hopes to have high community participation and succeed in reducing type II diabetes prevalence by 15%. TDPSMSP has put into consideration the social and economic barriers which could substantially affect the success of the program.
The program has SMART objectives in place which will be a guide to the success of TDPSMSP. The progress of the two groups will be based on their progress towards the set objectives. Use of social support and social cognitive approach unites the community to supporting each other, learning from each other and increasing their self- efficacy hence improving the chances of the program’s success.
References Cited
Agency for Health Care and Quality, (2001). Diabetes disparities among racial and ethnic Minorities. U.S. Department of Health and Human Services. Retrieved from http://www.ahrq.gov/research/diabdisp.htm#HighDiabetes
Calvin, D.J. (2012). African Americans’ perception of risk for diabetes complications. Neighborhoods Initiative. Retrieved from http://www.uic.edu/cuppa/gci/whatwedo/researchclusters/hcc/materials/Sharing%20What%20We%20Learn/2012/Donna%20Calvin%20Oct_Nov%20Featured%20Researcher.pdf
Castro, Shaibi & Boehm, (2009). Ecodevelopmental contexts for preventing type 2 diabetes in Latino and other racial/ethnic minority populations. EBSCO. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/detail?vid=15&sid=fc9ce4a3-4096-4a8a-a771-e732fecb03b5%40sessionmgr104&hid=118&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=aph&AN=36063457
Centers for Disease Control & Prevention, (2013). Take Charge of Your Diabetes. Retrieved from http://www.cdc.gov/diabetes/pubs/tcyd/ktrack.htm
Cheng, D. (2005). Prevalence, predisposition and prevention of type II diabetes. EBSCO. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/detail?vid=3&sid=05ffe02c-419c-48e5-887f-bcf239c0eb62%40sessionmgr198&hid=124&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=aph&AN=30094475
Engelgau, M. et al, 2004). The evolving diabetes burden in the United States. EBSCO. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/detail?vid=6&sid=963ddc38-8da7-46f7-b95b-cae149c0b514%40sessionmgr113&hid=118&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=aph&AN=13258281
Peek, Cargil & Huang, (2007). Diabetes health disparities. EBSCO. Retrieved from
http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/detail?sid=fc9ce4a3-4096-4a8a-a771-e732fecb03b5%40sessionmgr104&vid=16&hid=118
Simmons et al, (2013). Testing a peer support intervention for people with type 2 diabetes. BioMed Central Family practice. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/pdfviewer/pdfviewer?sid=df13c68c-ec81-416d-b75d-5c9322a53953%40sessionmgr113&vid=6&hid=122
Wishard, (2013). Community health centers. Retrieved from http://www.wishard.edu/our-services/community-health-centers
Wolf, S. et al, (2000). Controlling blood glucose levels in patients with type 2 diabetes mellitus. EBSO. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/detail?vid=5&sid=05ffe02c-419c-48e5-887f-bcf239c0eb62%40sessionmgr198&hid=124&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=aph&AN=3248690
Jiang, & Zhang(2012). Using social cognitive career theory to predict the academic interests and goals of Chinese middle vocational-technical school students. EBSCO. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/pdfviewer/pdfviewer?sid=3dfa5d96-d692-4c44-b51f-deb18113e297%40sessionmgr114&vid=6&hid=124
The next step is to teach the people already diagnosed with the disease, self- management skills. The aim of the self-management skills is to maintain blood glucose levels within normal levels. Normal blood glucose levels prevent diabetes related complications, hence diabetic people leading a normal healthy and productive life (Wolf, et al, 2000).
It is important to know the resources which are necessary for the success of TDPSMSP. The resources will be funding, which is an important component of the program. Without funding TDPSMSP will not take off. Funding sources will range from the state funding of TDPSMSP program, grants from foundations, Individual and organizational donations or a budget from the federal government. The funds will be used to pay the contracted research assistants, take care of the snacks and refreshments, purchase material for training and education, travel to the sites by researchers and any other expenses necessary to implement the program.
Other resource necessary for the TDPSMSP program are the training and education material. These include and are not limited to stationery, computers, projectors, the space to fit the participants, weighing equipment, blood glucose testing machines the accompanying accessories, training and education manuals among other material which might be required.
Human resource is another key component of the resources necessary to input into TDPSMSP. The human resources necessary to implement TDPSMSP include the pee supporters, the participants, researchers, the medical records staff, nurses, physicians, and dieticians. The researchers, peer supporters must work very closely with the Wishard community health center’s staff like the nurses, medical records staff and dieticians for TDPSMSP to succeed.
The activities involved will be the ones to help TDPSMSP take off. These activities will involve preparing the space for the classes, training peer supporters, enrolling the participants and preparing them for the program, preparing the training and educational material, ensuring that there is compliance with HIPAA during abstracting and partnering with the Wishard community health centers staff among others.
Upon completion of the activities, the TDPSMSP program will have made a lot of progress. The output will be implementation of the program in the 10 community health centers having trained peer supporters, having education manuals ready, prevention education on the 150 participants in progress and teaching the 150 participants self- management skills in progress.
The next step is very crucial for the TDPSMSP, because significant progress is expected at this stage. The outcome will depict either good or bad progress of TDPSMSP. The short term outcome will be the participants beginning to gain knowledge regarding type II diabetes disease and its risks. Participants will then take another step to begin healthy meal planning and physical exercises. For the long term output, significant results will be seen by participants making it a routine to eat healthy meals and exercise. In addition, substantial amount of weight will have been lost. The projected weight loss is 5% or greater of body weight. The participants BMI, blood pressure, cholesterol and blood glucose levels will be normal.
There will be a huge impact of TDPSMSP in the 10 communities implemented, based on the knowledge gained from the prevention education outreach. Participants and other community members will start seeking primary care where type II diabetes is screened and caught before it occurs. By the end of TDPSMSP period, 15% reduction in type II diabetes prevalence will be observed. There will be increased social support, a concept which started by utilizing peer supporters and instilling knowledge to the people in the community through the program. The community will also come together in collaboration to support each other to prevent and fight type II diabetes.
TDPSMSP is directly based on an evidence based program called “Testing a Peer Support Intervention for People with type II diabetes” (Simons, et al, 2013). This program had been implemented in England, United Kingdom in BioMed Central family practice. The program utilized peer support in type II diabetes management, whereby the peer supporters met with the participants and discussed the issues especially the challenges faced in living with type II diabetes. The peer supporters shared their experiences in living with the disease and the measures they had taken to succeed in self- managing type II diabetes. The peer supporters incorporated education during the discussions to help the participants learn type II diabetes self- management. The program had more shortcomings than advantages, although its concept is great, therefore it did not reap significant scientific results. This concept has been modified to fit in TDPSMSP implementation and will hopefully reap scientifically significant results.
The concept to utilize peer support has been adapted in TDPSMSP because the peer supporters are people who have had II diabetes for a long time. Their experience with the disease and the self- management skills will be a valuable asset in implementation and subsequent success of TDPSMSP. The peer supporters will practice active listening while conducting self-management forums. However, they will be guest speakers to the prevention group. The peer supporters will be role models to the participants. Most of the experiences the participants in the self-management group have been experiencing are the same ones the peer supporters experienced and the peer supporters will confirm that by sharing those experiences with the supporters. The participants will learn new skills from the peer supports on how to manage their blood glucose levels.
Further, the participants in the preventive group will learn by listening to the guest speakers who will be the peer supporters about the devastating experiences of dealing with type II diabetes. The aim of educating the preventive group using the peer supporters as guest speakers is not to instill fear but the reality about type II diabetes. The peer supporters will share about when they were clinically diagnosed and the type of lifestyle they lead before and after diagnosis. The preventive group will learn the importance of lifestyle change before it is too late, hence preventing type II diabetes.
TDPSMSP will be evaluated by reviewing the nutrition plans, weight, BMI, cholesterol and blood pressure of the preventive group on monthly basis. By the end of six months, the participants are expected to have normal BMI, cholesterol, blood pressure and having lost at 5% or greater of their body weight. For the self-management group, their blood sugar levels will be evaluated every 3 months using the summary lab test called the AIC test. This test has the ability to inform the healthcare provider about how much glucose on average, was stuck on a person’s hemoglobin for a period of 3-4 months. This test will tell if the self-management group is following the self-management skills they are being taught in their classes by the peer supporters. By the end of the 6 months period of TDPSMSP, the self-management group is expected to have lowered their glucose levels 6%-7%.
Contextual Factors
(Jiang & Zang, 2012) applied social cognitive theory to predict the academic interests and goals of Chinese middle vocational-technical school students. (Zhao, 2011) based the effects of the career choice consideration of Chinese farmers on the social support theory. TDPSMSP will also be based on social support and social cognitive theories.
The peer supporters who are part of the community where TDPSMSP will be implemented are social supporters. They are volunteering their time to support others who are also suffering from type II diabetes, to succeed in its management. Bringing the participants together in a discussion and education forums, is a way of encouraging support for each other. As participants continue to meet together, familiarity will lead to creation of relationships and in the process they will become each other’s social supporter. The preventive group is expected to support each other in meal planning and join hands in exercising together.
The participant’s self- efficacy, the ability to learn from the role models and their interest in the education material is the reason TDPSMSP is considered to be based on social cognitive theory. The self-management group is expected to learn the self-management skills from the peer supporters, who are also role models because they have succeeded in their blood glucose self-management. With time, the participants will also start learning from each other, for instance in the preventive group, there will be a few who will be doing very well in making healthy food choices and exercise. Their success will be seen in the amount of weight they lose each week, each month etc. Those lagging behind in this endeavor might improve by observing what their colleagues are doing, and they will try to do the same to succeed. The same case applies to the self-management group. Each week, each participant will be bringing their daily and weekly recordings of their blood glucose levels. Some of them will be doing so well and others will not have improved in self- management skills. The ones lagging behind will strive to do what the others are doing, in order to succeed in managing their blood glucose levels. The two groups’ efficacy will be based on their ability to face and act on the challenges of the program. Therefore, by the participants learning through observing the peer supporters or their fellow participants, the social cognitive theory comes into play. Also, other community members who are not participating in TDPSMSP are expected to learn and change their lifestyle by observing the TDPSMSP participants.
There are multiple factors which may negatively influence the success of TDPSMSP despite prior proper planning. Resistance from the community is a huge factor. If the community resists the program and fails to cooperative by participating and attending the classes as scheduled then TDPSMSP will not succeed. Also if there is high attrition of both participants and peer supporters, the program will fail. Participants are expected to stay in the program up to the end. If part of the cohort leaves before the program ends, then that will negatively affect the accuracy of the results. Another major factor is lack of enough funding. If the funding organizations or individuals do not continue to fund TDPSMSP, it will not be financially sustained to the end; therefore the effort will be futile. Harsh social economic factors whereby, the participants are not able to afford healthy nutrition because of low income due to joblessness, inability to participate in physical exercises outside of their homes due to bad physical terrain like bad or no sidewalks and unsafe neighborhoods, will also cause TDPSMSP to fail.
Race/ethnicity is another major factor and in this case having a project targeting only African Americans might be perceived as being biased. It might take a lot of program time to educate and explain why the program targets them. The researchers will have to explain how the African Americans are at higher risk than other minorities, but that does not guarantee their understanding.
Other factors which may positively influence the success of TDPSMSP include funding, whereby if funding is continued as promised, the program will succeed. Dedicated peer support is also a factor to consider. The researchers are banking on the peer supporters to support the two groups in meeting their set goals. Partnering with existing community health centers puts TDPSMSP at a very high chance of succeeding. When the participants realize how much interest the nurses, dieticians and their own doctors have in the success of this program, they will view it very important and they will be supportive as well. The site where the classes will take place is a familiar place in the neighborhood, which is their community health center. Therefore the participants will not experience a lot of change, because the healthcare professionals are the same familiar faces, the classes are taking place in a local area and the peer supporters are from their race and they probably know some of them.
Involving people in the community in a program that is targeting them, by basing the program on a social support and social cognitive theories, is a way of aiding TDPSMSP to succeed because it gives the participants a voice in their own program. It unites them as a community and makes them feel responsible and accountable for each other’s success indirectly.
Conclusion
Type II Diabetes Prevention and Self-Management Skills Program (TDPSMSP) was developed to target African Americans Adults aged 20 years and older, who have type II diabetes. TDPSMSP has a major objective to teach self-management skills to the community members who have been clinically diagnosed with type II diabetes and are struggling in maintaining healthy blood glucose levels. The program will also focus on prevention measures to reduce the prevalence of the disease by bringing awareness through education. TDPSMSP will utilize peer supporters, who are star patients because they have done well in self-managing their blood glucose to reasonably healthy levels. By working with peer supporters and partnering with Wishard‘s community health centers, TDPSMSP hopes to have high community participation and succeed in reducing type II diabetes prevalence by 15%. TDPSMSP has put into consideration the social and economic barriers which could substantially affect the success of the program.
The program has SMART objectives in place which will be a guide to the success of TDPSMSP. The progress of the two groups will be based on their progress towards the set objectives. Use of social support and social cognitive approach unites the community to supporting each other, learning from each other and increasing their self- efficacy hence improving the chances of the program’s success.
References Cited
Agency for Health Care and Quality, (2001). Diabetes disparities among racial and ethnic Minorities. U.S. Department of Health and Human Services. Retrieved from http://www.ahrq.gov/research/diabdisp.htm#HighDiabetes
Calvin, D.J. (2012). African Americans’ perception of risk for diabetes complications. Neighborhoods Initiative. Retrieved from http://www.uic.edu/cuppa/gci/whatwedo/researchclusters/hcc/materials/Sharing%20What%20We%20Learn/2012/Donna%20Calvin%20Oct_Nov%20Featured%20Researcher.pdf
Castro, Shaibi & Boehm, (2009). Ecodevelopmental contexts for preventing type 2 diabetes in Latino and other racial/ethnic minority populations. EBSCO. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/detail?vid=15&sid=fc9ce4a3-4096-4a8a-a771-e732fecb03b5%40sessionmgr104&hid=118&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=aph&AN=36063457
Centers for Disease Control & Prevention, (2013). Take Charge of Your Diabetes. Retrieved from http://www.cdc.gov/diabetes/pubs/tcyd/ktrack.htm
Cheng, D. (2005). Prevalence, predisposition and prevention of type II diabetes. EBSCO. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/detail?vid=3&sid=05ffe02c-419c-48e5-887f-bcf239c0eb62%40sessionmgr198&hid=124&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=aph&AN=30094475
Engelgau, M. et al, 2004). The evolving diabetes burden in the United States. EBSCO. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/detail?vid=6&sid=963ddc38-8da7-46f7-b95b-cae149c0b514%40sessionmgr113&hid=118&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=aph&AN=13258281
Peek, Cargil & Huang, (2007). Diabetes health disparities. EBSCO. Retrieved from
http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/detail?sid=fc9ce4a3-4096-4a8a-a771-e732fecb03b5%40sessionmgr104&vid=16&hid=118
Simmons et al, (2013). Testing a peer support intervention for people with type 2 diabetes. BioMed Central Family practice. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/pdfviewer/pdfviewer?sid=df13c68c-ec81-416d-b75d-5c9322a53953%40sessionmgr113&vid=6&hid=122
Wishard, (2013). Community health centers. Retrieved from http://www.wishard.edu/our-services/community-health-centers
Wolf, S. et al, (2000). Controlling blood glucose levels in patients with type 2 diabetes mellitus. EBSO. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/detail?vid=5&sid=05ffe02c-419c-48e5-887f-bcf239c0eb62%40sessionmgr198&hid=124&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=aph&AN=3248690
Jiang, & Zhang(2012). Using social cognitive career theory to predict the academic interests and goals of Chinese middle vocational-technical school students. EBSCO. Retrieved from http://web.ebscohost.com.proxy2.ulib.iupui.edu/ehost/pdfviewer/pdfviewer?sid=3dfa5d96-d692-4c44-b51f-deb18113e297%40sessionmgr114&vid=6&hid=124
